My brother in law told me at one point that he had sleep apnea.
The next week my boss, who never slept well and had a problem staying up in meetings, told me that he had sleep apnea and after having it treated he was really happy to be sleeping better and to be more rested all of the time.
Sleep Apnea is a very exhausting condition that causes you to wake up a bit all night long all the time so that you never get a restful night sleep.
A horrible thought for everyone and real hell if you are the one that is suffering from this.
What is Obstructive Sleep Apnea?
The most common kind of sleep apnea is called Obstructive Sleep Apnea Syndrome. Sleep apnea means “cessation of breath.” It is characterized by repetitive episodes of upper airway obstruction that occur during sleep, usually associated with a reduction in blood oxygen saturation.
In other words, the airway becomes obstructed at several possible sites. The upper airway can be obstructed by excess tissue in the airway, large tonsils, a large tongue and usually includes the airway muscles relaxing and collapsing when asleep.
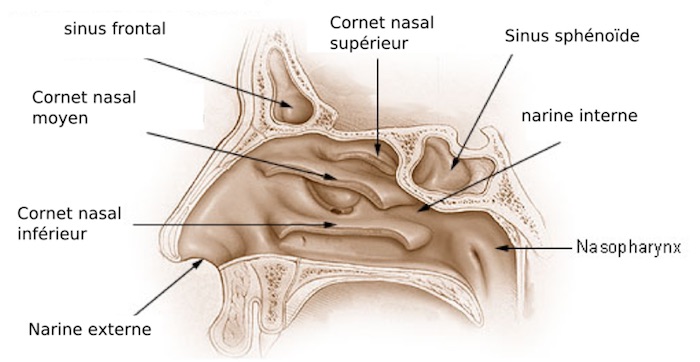
Another site of obstruction can be the nasal passages. Sometimes the structure of the jaw and airway can be a factor in sleep apnea.
What are the symptoms of Sleep Apnea?
- Excessive daytime sleepiness
- Frequent episodes of obstructed breathing during sleep. (The patient may be unaware of this symptom — usually the bed partner is extremely aware of this).
Associated features of Sleep Apnea may include:
- Loud snoring
- Morning headaches
- Unrefreshing sleep
- Dry mouth upon awakening
- Chest retraction during sleep in young children (chest pulls in)
- High blood pressure
- Over irritability
- Change in personality
- Depression
- Difficulty concentrating
- Excessive perspiring during sleep
- Heartburn
- Reduced libido
- Insomnia
- Frequent nocturnal urination (nocturia)
- Restless sleep
- Nocturnal snorting, gasping, choking (may wake self up)
- Rapid gain
- Confusion upon awakening
How Serious Is Sleep Apnea?
It is a potentially life-threatening condition that requires immediate medical attention.
The risks of undiagnosed obstructive sleep apnea include heart attacks, strokes, impotence, irregular heartbeat, high blood pressure and heart disease.
In addition, obstructive sleep apnea causes daytime sleepiness that can result in accidents, lost productivity and interpersonal relationship problems.
The severity of the symptoms may be mild, moderate or severe.
How Does the Doctor Determine If I Have Obstructive Sleep Apnea?
A sleep test, called polysomnography is usually done to diagnose sleep apnea. There are two kinds of polysomnograms.
An overnight polysomnography test involves monitoring brain waves, muscle tension, eye movement, respiration, oxygen level in the blood and audio monitoring. (for snoring, gasping, etc.)
The second kind of polysomnography test is a home monitoring test.
A Sleep Technologist hooks you up to all the electrodes and instructs you on how to record your sleep with a computerized polysomnograph that you take home and return in the morning.
They are painless tests that are usually covered by insurance, these will help you determine if an Obstructive Sleep Apnea Treatment is needed.
How is Sleep Apnea treated?
Mild Sleep Apnea is usually treated by some behavioral changes. Losing weight, sleeping on your side are often recommended.
There are oral mouth devices and other anti-snore device : sleep aid (that help keep the airway open) on the market that may help to reduce snoring in three different ways.

Some devices (1) bring the jaw forward or (2) elevate the soft palate or (3) retain the tongue (from falling back in the airway and blocking breathing).
Sleep Apnea is a progressive condition (gets worse as you age) and should not be taken lightly.
Moderate to severe Sleep Apnea is usually treated with a C-PAP (continous positive airway pressure). C-PAP is a machine that blows air into your nose via a nose mask, keeping the airway open and unobstructed.
For more severe apnea, there is a Bi-level (Bi-PAP) machine. The Bi-level machine is different in that it blows air at two different pressures.
When a person inhales, the pressure is higher and in exhaling, the pressure is lower. Your sleep doctor will “prescribe” your pressure and a home healthcare company will set it up and provide training in its use and maintenance.
Find out about the different manufacturers who provide respiratory equipment for obstructive sleep apnea.They have photos of their CPAP machines, masks and other equipment, so take a look.
Some people have facial deformities that may cause the sleep apnea. It simply may be that their jaw is smaller than it should be or they could have a smaller opening at the back of the throat.
Some people have enlarged tonsils, a large tongue or some other tissues partially blocking the airway. Fixing a deviated septum may help to open the nasal passages.
Removing the tonsils and adenoids or polyps may help also. Children are much more likely to have their tonsils and adenoids removed.
Tracheostomy
The only available treatment until the early 1980’s was a tracheostomy. A tracheostomy is a surgical procedure where a small hole is cut in the neck and a tube with a valve is inserted into the hole.
During the day the valve is closed so the person can speak. At night, the valve is opened, thus avoiding the obstructions.
This procedure is only used today as a last resort or to avoid respiratory distress, or other serious medical complications (You would have to be extremely sick to require this).
Uvulopalatopharyngoplasty (UPPP)
What is available today in the way of surgery is the uvulo-palato-pharyngoplasty (UPPP). What does this mean?
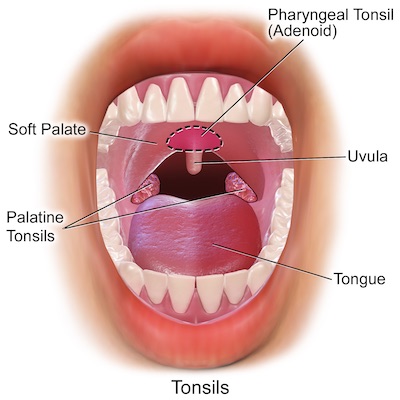 The uvulo refers to the uvula, that fleshy thing hanging in the back of your throat, palato refers to the palate, and pharyngoplasty means plastic surgery of the pharynx (the pharynx is the joint opening of the gullet and the windpipe).
The uvulo refers to the uvula, that fleshy thing hanging in the back of your throat, palato refers to the palate, and pharyngoplasty means plastic surgery of the pharynx (the pharynx is the joint opening of the gullet and the windpipe).
The uvula is removed along with excess tissue. This surgery is usually done for patients who can’t tolerate nasal CPAP.
This surgery has mixed reviews, it helps in around 50% who have the surgery and in others it does not help at all or it helps only partially and the patient may still need to use the C-PAP machine due to scar tissue.
Mandibular Myotomy
A procedure called mandibular myotomy was crafted by Drs. Nelson Powell and Robert W. Riley who are associated with the Stanford University Sleep Disorders Center.
This procedure, mandibular myotomy ( mandibular = relating to the lower jaw bone, and myotomy = surgical division of a muscle) with genioglossis (chin and tongue) advancement, involves cutting a rectangular piece of bone in the anterior (front part) portion of the mandible (jaw) to which the tongue muscles are attached.
At that point, the rectangular piece is pulled outward, rotated 90 degrees and attached so it overrides the defect produced by the osteotomy (cutting of bone), where it is reattached. This pulls the tongue forward six to ten millimeters and almost always eliminates the sleep-related obstruction.
These surgeries requires much research and consideration before you undertake it. They should only be performed by surgeons with considerable experience and documented training and skill in both ENT surgery and maxillofacial surgery.
Laser Assisted Uvuloplasty (LAUP)
There is also Laser Assisted Uvuloplasty (LAUP), is a surgical procedure to remove the uvula and surrounding tissue to open the airway behind the palate. This procedure has been used to relieve snoring. It has been used somewhat successfully in treating sleep apnea. Always make sure you have a doctor who has done the procedure many times and is preferrably extremely knowledgeable about sleep apnea. Ask lots of questions and do your homework!
Radiofrequency (RF) Procedure or Somnoplasty
The newest surgical procedure for snoring and sleep apnea is called somnoplasty. The U.S. Food and Drug Administration has approved a treatment for snoring that uses radio waves to shrink tissue in air passages and eliminate snoring.
The procedure is called radiofrequency volumetric tissue reduction of the palate.
A new treatment for sleep apnea, radio frequency volumetric reduction of the tongue has been approved by the FDA.
The radiofrequency treatment involves piercing the tongue, throat or soft palate with a special needle (electrode) connected to a radio frequency generator.
The inner tissue is then heated to 158 to 176 degrees, in a procedure that takes approximately half an hour.
The inner tissues shrink, but the outer tissues, which may contain such things as taste buds, are left intact. Several treatments may be required.
Unfortunately, at this time the procedure is so new that insurance companies are not covering it yet. It is still seen as an experimental procedure.
Nasal Obstruction
Sometimes the nasal passages are a site of obstruction. It can be from a deviated septum, large turbinates (nasal bones) or a collapse of the nostril area, called the nasal valve.
The Radiofrequency procedure (see above) can effectively reduce the size of the turbinates. Septoplasty surgery can fix a deviated septum and nasal valve surgery will take care of nostril collapse.
Oral Positive Airway Pressure (OPAP)
Another new invention that is being tested is the OPAP, a dental appliance that conducts air through it (interesting info starts on third page of that link – a little dense as well). It may prove to be to be an alternative to the mask and headgear.

This is the apparatus that my boss used. What it does is move the lower jaw forward and has a screw in it that allows you to move the jaw forward to a comfortable position.
Of course this is only worn while you sleep and after the first night is apparently comfortable enough to sleep with.